
In a recent post, I wrote about how the field of sexology is uneven in its application and rife with regional and individual biases, largely due to general sex phobia and a subsequent lack of empirical research within the field. Recently, a debate on the mailing list of one of the sexological organizations to which I belong touched again upon discrepancies within the field. The discussion in question concerned whether or not it is possible to eradicate a fetish. Most respondents were in agreement that, like a sexual orientation, eradicating a sexual fetish is not only not possible, but particularly in fetishes that cause no harm, even unethical.
One clinician, however, stated not only that eradicating a fetish is possible, but then went on to describe exactly how (he/she believes) it is done. The methodology described was so disturbing, however, that I felt it necessary to challenge the ideas presented and to present both his/her perspective as well as my response here on my blog as a cautionary tale to individuals who may have questions regarding their own sexuality so that the know what to avoid in therapy. I have eliminated any details that could reveal the identify of the other clinician.
Below is what the clinician wrote in support of fetish eradication. I am highlighting and italicizing the most objectionable aspects:
I don’t see a fetish as similar to sexual orientation – it is something that does reflect “something wrong”, and in my own experience, DOES respond to therapy! One issue is that sexual fetishes – paraphilias – typically involve sexual activity with something that does not provide the rewards that sex with another human does. That is, talking, kissing, caressing, oral sex, intercourse, etc. Compared to these things, really, what does masturbating while doing something like holding on to a shoe, cross dressing, etc. have to offer? In the cases I have had good results with, I have used some combination of procedures to reduce the arousal value of the fetishistic practice; and, at least as importantly, procedures to make good, open, rewarding sexual activity with a consenting adult available to the patient. This procedure has seen been termed “cognitive negative conditioning”. Sometimes this been done with the patient sniffing disgusting aromas or unpleasant chemical agents, but I long ago stopped doing this, and went to the strictly cognitive negative conditioning procedures. The reason for this was that I had a patient confess that he had indeed used all 7 of his ammonia vials this week – but he had broken them out in the parking lot just prior to coming in to see me!
The “cognitive negative conditioning procedures” involve having the patient spend….
time thinking about – and saying into the small tape recorder I give the patient -all the things that are now going wrong in his life because of his fetish; and what is likely to happen in the future for him, because of his fetish, really does reduce the arousal value of the fetish – and this is something that can’t be done in a couple of minutes, on just one day. One thing I have also found often really strongly effective as a negative involves children, if the patient has any. For example, I had one man who had a shoe fetish think about his children coming home from school in tears, saying how they were being teased about “What a freak your old man is – him and his shoe —— (expletive deleted). In another case, we arrived at the man’s daughter saying her boyfriend was now forbidden to date her anymore: “His parents said, ‘Come on, his Dad is some kind of a weirdo pervert!’ Oh Dad, how could you do this to me?”
Further….
While I always do the cognitive conditioning procedure with fetish patients, I sometimes also do the “stimulus satiation procedure”, which involves changing the patients masturbation. This is not something I usually use – it is reserved for patients who have what might be called an “extreme” fetish, and are also very well motivated. This procedure involves having the patient (at home, of course) masturbate using normal – non-fetish- stimuli/fantasy. Immediately after reaching orgasm, the man switches to his fetish, and continues to masturbate, without stopping, for a time that is unpleasant- I usually start the man with something like 10 or 15 minutes. During this time, the man will lose his erection; will not be aroused; and will likely find it painful. Should any pleasure/arousal occur, he must immediately switch back to NORMAL stimuli. The major problem here is that it is some of the wives of the man with a fetish (I don’t think I am being sexist here; I just don’t recall ever seeing a female with what could be considered a genuine “fetish”) are so distressed by learning about his fetish that their interest/ability in sexual functioning with him are severely reduced. I have found some success with this problem by putting off this part of the problem until we can say that his interest in the fetish is genuinely gone.
So basically if someone shows up to this therapist with questions or concerns about a fetish, the patient will be subjected to shameful thoughts and experiences regarding his own children and will be pushed into unpleasant and painful physical sensations. Wonderful. Where can we all sign up? Look, whatever this therapist is up to is not only cruel and unusual, but according to the new changes in the DSM 5, in which paraphilias (fetishes) were de-pathologized, also highly unethical. New studies keep being published showing that fetishes are not correlated to pathology. And this person considers himself a sexologist and sex therapist. This sex phobia and negativity must be stopped, especially in clinical settings, before more unwitting people put their trust in ignorant practitioners and get hurt. There is a word for illness cause by doctors– iatrogenic. My call to the mental health field: No more iatrogenic harm to patients around issues of sexuality.
Below is my reasoned response (which went unanswered):
Do you have any empirical evidence for the efficacy of your negative conditioning and aversive techniques for fetishes? Do you have supporting documentation on what percentage of fetishes “prevent, good, open rewarding sexual activity with a consenting adult”? Many of the clients I’ve seen who have discussed their fetishes have described them in ways that enhance, rather than diminish, their sexual functioning with consenting adults. And I’m also wondering why, when working with distressed wives of the fetishist, your first option appears to eradicate the fetish rather than help the wife process her distress and understand more about the fetish, as well as take a systemic look at what else is going on in the relationship. It also appears that you are lumping all fetishes together, including those that are merely optional, preferred, as well as exclusive. Are you aware that the DSM 5 differentiates between paraphilias (which are not pathological) and paraphilic disorders?














































































 Prevention: Is Sex Addiction Real?
Prevention: Is Sex Addiction Real? Fatherly: BDSM More Common Than You Think
Fatherly: BDSM More Common Than You Think Who Magazine: What is Bisexuality?
Who Magazine: What is Bisexuality?
 Great article in Prevention Magazine about the sex addiction controversy. Check out what I had to say.
Great article in Prevention Magazine about the sex addiction controversy. Check out what I had to say.
 Interesting piece in Fatherly about BDSM in which I was interviewed.
https://www.fatherly.com/love-money/bdsm-kinky-sex-not-uncommon/
Interesting piece in Fatherly about BDSM in which I was interviewed.
https://www.fatherly.com/love-money/bdsm-kinky-sex-not-uncommon/ Who is Australia's version of People Magazine. They wanted to know what bisexuality is and I provided some insight.
Who is Australia's version of People Magazine. They wanted to know what bisexuality is and I provided some insight.
 I answer questions from Salon.com about the infamous porn site PornHub.
I answer questions from Salon.com about the infamous porn site PornHub.
 I am interviewed in this fairly nuanced piece on the pros and cons of porn.
I am interviewed in this fairly nuanced piece on the pros and cons of porn.
 I am interviewed in this intriguing Business Insider article on how often happy couples have sex.
I am interviewed in this intriguing Business Insider article on how often happy couples have sex.
 The Huffington Post in South Africa profiles my work around challenging sex addiction (including my red/yellow/green menu exercise) .
The Huffington Post in South Africa profiles my work around challenging sex addiction (including my red/yellow/green menu exercise) .
 I give some insight into this interesting topic.
https://thetab.com/us/2017/03/22/happens-boyfriend-leaves-another-man-63306
I give some insight into this interesting topic.
https://thetab.com/us/2017/03/22/happens-boyfriend-leaves-another-man-63306 I give Redbook some pointers on having a 3some for the first time.
I give Redbook some pointers on having a 3some for the first time.
 I am featured in this terrific New York Magazine article, discussing some of the finer points brought up in the earlier article in SELF magazine (see listing below).
I am featured in this terrific New York Magazine article, discussing some of the finer points brought up in the earlier article in SELF magazine (see listing below).
 Complex asked me to weigh in on this provocative topic.
Complex asked me to weigh in on this provocative topic.

 I weigh in in this great advice column in Thrillist by Elle Stanger.
I weigh in in this great advice column in Thrillist by Elle Stanger.

 Great episode, check it out.
https://soundcloud.com/futureofsex/04-exploring-sexual-fluidity-bicuriousity-for-women-featuring-skirt-club-and-dr-michael-aaron
Great episode, check it out.
https://soundcloud.com/futureofsex/04-exploring-sexual-fluidity-bicuriousity-for-women-featuring-skirt-club-and-dr-michael-aaron In this episode, we talk about the societal myths of sexuality, including:
In this episode, we talk about the societal myths of sexuality, including:
 I was asked to appear on Australian radio. It was a very fun segment, will post the link when I have it!
I was asked to appear on Australian radio. It was a very fun segment, will post the link when I have it! I appear on the Stereo-Typed podcast to discuss my new book, fantasies, and our shadow self. Click the audio player below and enjoy!
https://www.spreaker.com/user/crazyheart/stereo-typed-8-dancing-with-your-shadow
I appear on the Stereo-Typed podcast to discuss my new book, fantasies, and our shadow self. Click the audio player below and enjoy!
https://www.spreaker.com/user/crazyheart/stereo-typed-8-dancing-with-your-shadow I appear on the Boom Doctors Podcast to discuss my new book Modern Sexuality and my work as a sex therapist. Clink the link below to listen in.
http://theboomdoctors.com/2016/09/21/ep-132-michael-aaron-on-his-work-as-a-sex-therapist-his-new-book-modern-sexuality/
I appear on the Boom Doctors Podcast to discuss my new book Modern Sexuality and my work as a sex therapist. Clink the link below to listen in.
http://theboomdoctors.com/2016/09/21/ep-132-michael-aaron-on-his-work-as-a-sex-therapist-his-new-book-modern-sexuality/ I appeared on French national tv channel Canal + on the Emission Antoine tv show, discussing the psychology behind financial domination. I will post a video clip of the interview shortly.
I appeared on French national tv channel Canal + on the Emission Antoine tv show, discussing the psychology behind financial domination. I will post a video clip of the interview shortly. I was interviewed on Huffington Post's Love + Sex Podcast, which I'm told is the most downloaded sex and relationship podcast on iTunes. In this episode, I dispel the wild myths about "sex roulette" parties.
I was interviewed on Huffington Post's Love + Sex Podcast, which I'm told is the most downloaded sex and relationship podcast on iTunes. In this episode, I dispel the wild myths about "sex roulette" parties.
 I was interviewed for an upcoming online sexuality discussion series, the Sexual Reawakening Summit. It features many top sex therapists from around the country and you can access it by using this link:
I was interviewed for an upcoming online sexuality discussion series, the Sexual Reawakening Summit. It features many top sex therapists from around the country and you can access it by using this link:  In the April edition of my Men's Fitness 'Sex Files' Q&A column, I answer questions about anal sex and porn. Hurry and pick up a copy before it's off the stands!
In the April edition of my Men's Fitness 'Sex Files' Q&A column, I answer questions about anal sex and porn. Hurry and pick up a copy before it's off the stands!

 Looks like Yahoo News picked up the Reuters article on women's fears that their partners expect sexual perfectionism. Check it out.
Looks like Yahoo News picked up the Reuters article on women's fears that their partners expect sexual perfectionism. Check it out.
 My latest interview with Reuters, this time about social pressure on women to be perfect sexually. "Our society is filled with sexual myths and misconceptions, mostly stemming from a combination of our culture's puritanical roots, as well as rampant consumerism, which feeds off individual insecurities to sell unnecessary products," Aaron said.
My latest interview with Reuters, this time about social pressure on women to be perfect sexually. "Our society is filled with sexual myths and misconceptions, mostly stemming from a combination of our culture's puritanical roots, as well as rampant consumerism, which feeds off individual insecurities to sell unnecessary products," Aaron said.
 Want to know more about what the AltSex NYC Conference is all about? I appear with my co-organizer, Dulcinea Pitagora, on the Sex with Timaree show, a popular podcast, to discuss numerous things including how the conference was created and what attendees can expect. Click on the link below to check it out:
https://sexwithtimareepodcast.wordpress.com/2016/02/29/ep236-the-upcoming-alt-sex-nyc-conference-sex-with-timaree-altsexnyc-2/
Want to know more about what the AltSex NYC Conference is all about? I appear with my co-organizer, Dulcinea Pitagora, on the Sex with Timaree show, a popular podcast, to discuss numerous things including how the conference was created and what attendees can expect. Click on the link below to check it out:
https://sexwithtimareepodcast.wordpress.com/2016/02/29/ep236-the-upcoming-alt-sex-nyc-conference-sex-with-timaree-altsexnyc-2/ Head out to the newsstands and grab a copy of the Jan 2016 issue of Men's Fitness Magazine to see the premier of the new monthly "Sex Files" column in which I answer readers' sex questions. In this month's issue I answer a question in which a guy is looking to help his girlfriend enjoy more pleasure when she is having sex on top. Check out the screenshot below to see my response:
Head out to the newsstands and grab a copy of the Jan 2016 issue of Men's Fitness Magazine to see the premier of the new monthly "Sex Files" column in which I answer readers' sex questions. In this month's issue I answer a question in which a guy is looking to help his girlfriend enjoy more pleasure when she is having sex on top. Check out the screenshot below to see my response:

 Love& is a new magazine about relationships and sex. They interviewed me about common things that women may want their guys to improve upon in the bedroom. One of the big ones is touch, as a lot of men are way too rough and don't know how to adjust their touch to what their partner wants. For more on this, and other pointers, check out the article itself below:
Love& is a new magazine about relationships and sex. They interviewed me about common things that women may want their guys to improve upon in the bedroom. One of the big ones is touch, as a lot of men are way too rough and don't know how to adjust their touch to what their partner wants. For more on this, and other pointers, check out the article itself below:
 Does Bill Cosby have a fetish for unconscious women? Who knows? He's not a client and I've never met him, so I cannot say for sure, but this provocative piece in the NY Times tries to get to the bottom of his alleged bizarre behavior. The reporter did a great job dealing with some uncomfortable material, so be sure to click the link below to see what I had to say on this issue:
Does Bill Cosby have a fetish for unconscious women? Who knows? He's not a client and I've never met him, so I cannot say for sure, but this provocative piece in the NY Times tries to get to the bottom of his alleged bizarre behavior. The reporter did a great job dealing with some uncomfortable material, so be sure to click the link below to see what I had to say on this issue:
 I was recently asked by a reporter from Men's Fitness magazine to discuss reasons why a heterosexual man might refrain from having sex with a willing woman. The questions were basically soft balls, seemingly aimed at a younger, more inexperienced, male audience, but hey, I managed to drop a few decent pointers, relating to finding out if the woman is in a relationship, and if so, what kind of relationship she is in before diving in. If you want to take a look and poke around more, you can go directly to the article below. You are going to have to click to page 3 to see my quotes, btw.
I was recently asked by a reporter from Men's Fitness magazine to discuss reasons why a heterosexual man might refrain from having sex with a willing woman. The questions were basically soft balls, seemingly aimed at a younger, more inexperienced, male audience, but hey, I managed to drop a few decent pointers, relating to finding out if the woman is in a relationship, and if so, what kind of relationship she is in before diving in. If you want to take a look and poke around more, you can go directly to the article below. You are going to have to click to page 3 to see my quotes, btw.
 I was recently interviewed for a Men's Health article on sex toys designed for men. They wanted to know my take on these "robotic masturbators" (as they called them) and as always, I tried to take a fair and balanced view of things. I pointed out that they could be used as a way to get better acquainted with one's sexuality (as well as get some much needed relief), but an over-reliance on technology may also limit guys from developing the necessary skills that would help them form romantic relationships.
At any rate, hurry on over to the article here--
I was recently interviewed for a Men's Health article on sex toys designed for men. They wanted to know my take on these "robotic masturbators" (as they called them) and as always, I tried to take a fair and balanced view of things. I pointed out that they could be used as a way to get better acquainted with one's sexuality (as well as get some much needed relief), but an over-reliance on technology may also limit guys from developing the necessary skills that would help them form romantic relationships.
At any rate, hurry on over to the article here-- 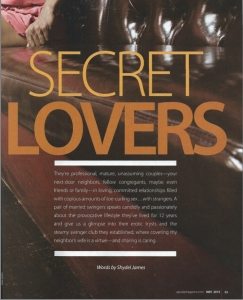 Go check out a great, and I mean GREAT, absolutely fascinating article in the May issue of Upscale Magazine, entitled "Secret Lovers," in which I am interviewed regarding the hush hush world of the swinger subculture. The writer does a really good job of trying to understand the psychology of folks who practice consensual non-monogamy and I think the piece is very even-handed, with some practical tips for couples who are curious about dipping their toes in the lifestyle. I'll leave you with a quote from one of the swingers profiled in the piece, which I think gives a good feel for the tone and depth of the article-- "I love to see her with two guys and two girls at once. I enjoy submissive women, and there is no sexier submission than to watch my wife please me by pleasing others." If that sounds interesting, then I suggest you head out and grab a copy. It's well worth the read.
Go check out a great, and I mean GREAT, absolutely fascinating article in the May issue of Upscale Magazine, entitled "Secret Lovers," in which I am interviewed regarding the hush hush world of the swinger subculture. The writer does a really good job of trying to understand the psychology of folks who practice consensual non-monogamy and I think the piece is very even-handed, with some practical tips for couples who are curious about dipping their toes in the lifestyle. I'll leave you with a quote from one of the swingers profiled in the piece, which I think gives a good feel for the tone and depth of the article-- "I love to see her with two guys and two girls at once. I enjoy submissive women, and there is no sexier submission than to watch my wife please me by pleasing others." If that sounds interesting, then I suggest you head out and grab a copy. It's well worth the read.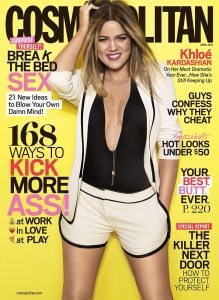 I am featured in the Sex Q&A section of Cosmo's April 2014 issue, in which I get asked about BJs, Plan B, sex in hot tubs, and all kinds of other tittilating reader questions. They did a good job of adding all kinds of humor, including a silly picture of tea bags-- need I say more? It's a can't- miss hoot. Go and check it out at news stands now!
I am featured in the Sex Q&A section of Cosmo's April 2014 issue, in which I get asked about BJs, Plan B, sex in hot tubs, and all kinds of other tittilating reader questions. They did a good job of adding all kinds of humor, including a silly picture of tea bags-- need I say more? It's a can't- miss hoot. Go and check it out at news stands now!{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Please email me the name of this therapist. My fetish is disabling and hurtful in that it makes it difficult for me to have a relationship with another human being. My fetish also causes me to produce estrogen and excess cortisol, which has an immediate and tangible negative effect on my ability to deal with anxiety. Any therapist who cares about my quality of life would respect my decision … Again, please email me the name of this therapist!
I’d like the email of that therapist.